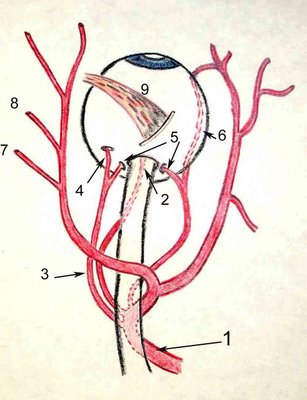
The blood supply to the choroid comes ultimately from the ophthalmic artery (#1 in figure). There are variations but quite posterior branches will become the central retinal artery (#2 in Figure), and ciliary arteries (#3 in Figure) on each side of the optic nerve. These vessels divide into 2 long posterior ciliary arteries(#4 in Figure) and ~20 short posterior ciliary arteries (only one on each side is shown in the diagram #5 in Figure) that enter the eye immediately adjacent and around the optic nerve. The short posterior ciliary arteries directly supply the choroid and the long posterior ciliary arteries travel in the suprachoroidal space anteriorly (#6 in Figure) then supply the choroid anteriorly via recurrent branches. The ophthalmic artery (#1 in Figure) continues to provide branches for the posterior (#7 in Figure) and anterior (#8 in Figure) ethmoidal vessels. The superior oblique muscle is shown for orientation ( #9 in Figure).
Blood in the choroid circulates through the choriocapillaries and larger vessels of the choroid to drain into 4-6 vortex veins.

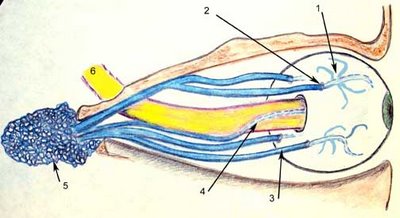
In the photograph of a transilluminated portion of the eye in which the retina has been cut away the whorled vortices of the choroidal veins are evident as they coalesce and drain into a single vortex vein. (Also see #1 in Figure drawing). The vortex veins emerge just posterior to the equator (#2 in Figure) in quadrants. The superotemporal and superonasal (#1 and 2 in Figure) vortex veins will drain into the superior ophthalmic vein. The inferonasal and inferotemporal vortex veins will drain into the inferior ophthalmic vein. These vessels will eventually exit via the cavernous sinus (#5 in Figure).
The vortex veins anastomose with the anterior ciliary veins (not shown in the figures). The anterior ciliary veins normally carry blood only from the anterior ciliary muscle, but if the vortex veins are occluded (e.g. from a poorly placed scleral buckle) the anterior ciliary veins may become quite dilated.
The superotemporal ophthalmic vein usually exits the eye directly adjacent to or underneath the superior oblique tendon. This has clinical implications for approaches to surgery in which the superior oblique tendon is recessed. Note that the superior ophthalmic vein moves inferiorly and temporally to exit the eye in the superior orbital fissure. This anatomic feature is important when evaluating radiologic studies for carotid cavernous fistula in which the superior ophthalmic vein is enlarged. The inferior ophthalmic vein is said to pass thru the inferior orbital fissure in section 2 of the BCSC. This may not be correct. Most texts show that it either communicates with the pterygoid plexus in the inferior orbital fissure but then either joins the superior ophthalmic vein or exits separately through the superior orbital fissue.
The circulation of the anterior portion of the eye features an intricately anastomotic system that essentially join the anterior ciliary circulation and the long posterior ciliary circulation in 3 interconnected arterial circles, an episcleral circle where episcleral vessels join, an intramuscular ciliary circle and the major arterial iris circle (
circumferential vessels in the ciliary body). The anterior ciliary venous system joins conjunctival and episcleral vessels at the limbus.
This ends the required information for UCLA students taking the one week required clerkship in Ophthalmology. All others please continue. UCLA OP-264.01 students and Jules Stein residents please continue with the
ocular pathology tutorial.
<
NEXT TUTORIAL OCULAR PATHOLOGY>
